




Epidemiological analysis and patterns of disease amongst patients hospitalized with dengue infection across different hospitals in India
- Part 3 -
Dr. Laishram Ranbir *
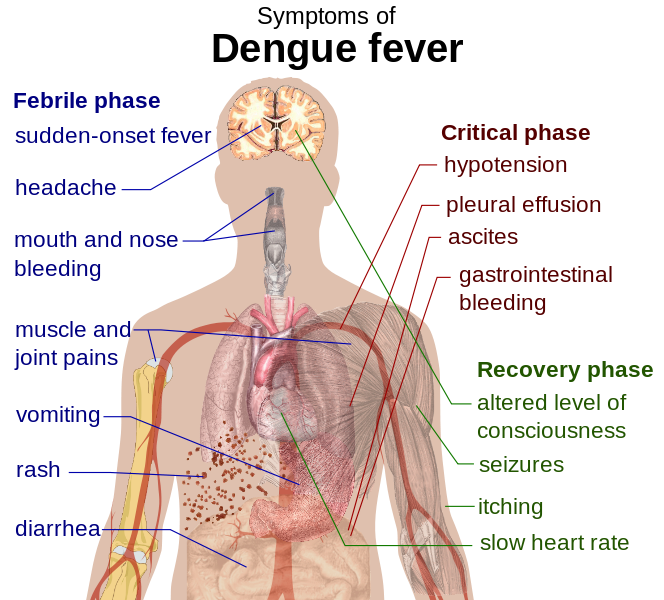
Main symptoms of dengue fever :: Pix - Wikipedia/Mikael Häggström
B.K. Tyagi.1, S. Karthigai Selvi 1, C. Vidya 1, T. Mariappan 1, P. Philip Samuel 1, R. Paramasivan 1, Mukul Gaba 2, N.K. Arora 2, S. Vivek Adhish 3, Deoki Nandan 3, Donald S. Shepard 4, Yara Halasa 4, Harish K. Pemde 5, Anurag Tomar 6, Poovazhagi Varadarajan 7, Pawan Kumar 8, Ashok Mishra 9, V.K. Srivastava 10, Koushik Vyas 11, Ranbir L. Singh 12, Bhadresh R.Vyas 13, Pallavi Shelke 14
1 Centre for Research in Medical Entomology (ICMR), 4-Sarojini Street, Chinna Chokkikulam, Madurai 625002, TN, India (Email: [email protected])
2 National Institute of Health & Family Welfare, Munirka, New Delhi
3 INCLEN Trust International, Okhla Industrial New Delhi
4 Brandeis University, 415 South Street, MS 035, Waltham, MA, USA
5 Lady Harding Medical College, New Delhi
6 NIMS Medical College, Rajasthan
7 Madras Medical College (Institute of Child Health), Tamil Nadu
8 Kasturba Medical College, Karnataka
9 G.R. Medical College, MP
10 IIMS R, UP
11 SCB Medical College, Odisha
12 RIMS, Manipur
13 M.P.Shah Medical College, Gujarat
14 LTM Medical College & General Hospital, Maharashtra
Correspondence to
Dr.B.K.Tyagi
Centre for Research in Medical Entomology (ICMR),
# 4, Sarojini Street, ChinnaChokkikulam,
Madurai-625 002, Tamilnadu, India.
Tel: + 91 452 2520565;
Fax:+ 91 452530660.
Email:[email protected]
Laboratory Investigation
The mean hematocrit in our study was 36.71gm % (SD=7.46). More than 40% of hematocrit was observed in 198 (31.9%) cases.The median platelet count was 58000/cu mm. A platelet count of < 1 lakh cells/cu mm was observed in 75.22% among the dengue cases. Platelet count of < 1 lakh/cu mm was seen 72.5% and 78.7%among children and adult patients, respectively.
The mean alanine aminotransferase (ALT) in dengue suspect and dengue probable was 130.33 U/L, and166.91 U/L, respectively. About 60.10% of patients had mild elevation of ALT (49.5% of dengue suspect, and 64.3% of dengue probable). Elevation of ALT above 200 U/L was found in 16% of dengue cases where dengue suspect and probable was 9.9% and 18.5% respectively.The mean aspartate aminotransferase (AST) in dengue suspect and probable patients was 99.68 U/L and 217.19 U/L, respectively. About 77.93% of dengue suspect/probable patients had elevation of AST, out of which 52.1% had mild elevation (50.3% of dengue suspect and 52.8% of dengue probable). Elevation of AST > 200 U/L was found in 25.8% of dengue patients.
Screening Test
NS1 test was not commonly used in early identification but was done for only96 (6.62%) patients, out of which 38.54% was positive. The test conducted for 10 cases (10.42%) of dengue patients among the total NS1 test doneweredone after 6-12 days of illness which yielded negative result for whom the other laboratory confirmatory tests were not performed. It was usedinnegligible proportion in North, central and southern region compared to other regions. The standardized dengue enzyme linked immunosorbent assay (ELISA)IgM was the test most commonly used and done for about 1054 (72.69%) of cases with suspicion of dengue, out of which 88.67% of dengue probable patients were positive. IgG test was positive in about 25.59% of dengue probable.
Discussion
This study reports the results of the selected hospitals based on region wise. The study sample of cases were recruited based on the discharge with clinical diagnosis of DF, DHF and DSS and then careful classification of diagnosis was done according to the WHO's guidelines of DF/DHF/DSS33. It was found that thoughall the cases with discharge diagnosis of DF/DHF/DSS based on Indian scenario met the clinical criteria of WHO's guidelines of DF/DHF/DSS but it did not comply with the laboratory criteria specified under the guidelines for confirmed DF/DHF/DSS, hence all the cases were reclassified under Dengue suspect and probable based on fulfillment of clinical and laboratory test specified in the WHO guidelines.
In this study, southern region contributed around 41.12% of hospitalized cases. Sex distribution shows a male predominance inthe study and this finding is in concordancewith thatof an earlier study 34-35. The proportion of dengue cases forthe age group of 15-44 was highest which is consistent with other Indian studies25, 36 and geriatric population was lowest but registered with high mortality rate of 14.29% next to which comes the Infants (0-1 year) contributes to 8.6%. In a retrospective study of the 1981 DHF outbreak in Cuba, peak mortality rates were observed in children and in adults above 60 years old 37. The mean age of the dengue cases (admitted in general hospital) was 28 years, indicating that the majority of cases are in productive working age.In this study it was noted that the adult population was also being highly affected equally by dengue infection compared to child population during the study period. This age shift is clearly observed, indicating an epidemiological change in dengue infection38
Dengue has traditionally been viewed as a disease of high population density tropical urban areas39. However, in our study, it was found that about 43.86% of hospitalized dengue cases from rural areas, mainly reported from some part of northern and southern region in India. The factors accountable for transition/shift of dengue illness might be due to the water storage practices; increased awareness of dengue reflects in better health seeking behavior and also due to developmental activities taken place in rural areas. The seasonal trend of dengue cases hospitalized was also noticed in this study. Dengue infection and its mortality rate were reported throughout the year but it gradually increased during pre and post monsoon season with a peak level in October during the study period (2006-2011). It indicates that the rainfall and temperature favoured high rates of mosquito breeding/reproduction40.Factors responsible for incidence of dengue fever throughout the year need to be identified.
The average duration of fever before admitting into study sites, duration of hospitalization, and total duration of illness episode through discharge for dengue patients were 6.51 days (+ 5.1), 5.67 nights (+ 4.11) and 12.17 days (+ 4.11). Comparison of clinical features between children and adult population indicates that the children had experienced higher and greater severity of thrombocytopenia, shock, liver and spleen enlargement, vomiting, abdominal pain, pleural effusion and ascites which may be the leading cause of high mortality.
The tourniquet test is a key parameter as it is the only hemorrhagic manifestation seen in dengue fever. In this study, the test was positive in 17 cases (13.08%) of the 130 (9%) on whom it was done. It was found that the test was not highly effective in notifying the symptoms of petechiae and severe bleeding. This finding is in conformity with the observations of other studies41-43
The main effect of a reduced platelet count is an increased risk of bleeding. In the study, it was found that the platelet count was less than 1 lakh in 1026 (75.22%) of the 1364 cases who have tested. About 269 (36.50%) of 1026 cases who have less than 1 lakh platelet count, were reported to have bleeding manifestation such as petechiae, haemetemesis, severe bleeding and malena. Although thrombocytopenia was a common finding, there was poor correlation between thrombocytopenia and bleeding tendencies, the similar finding was also observed in other studies44-47. About 46 (3.41%) of patients were marked severe thrombocytopenia with a platelet count < 10,000 cells/mm. Among those around 13 (37.14%) had petechiae, haemetemesis, severe bleeding or malena. Liver enlargement is a common finding which goes hand in hand with other studies with moderate to peak elevation of ALT/AST. Elevated liver enzymes with thrombocytopenia are known to be an early warning sign for severe bleeding which was clearly observed in the study.
Conclusion
Our study shows that a lot of dengue cases might be missed under the current definition of dengue, since they are not necessarily subjected to confirmatory laboratory investigations. Dengue being referred as a paediatric disease is now clearly showing a shift towards the adult population, particularly geriatrics accounting for high mortality. The difference in infection rate is high in males than females which conform to similar observations by others both in India and Singapore48-50. Even though the morbidity is high among males the mortality rate is high in the females (5.11%) when compared to that of males (3.8%) which is also corroborated by another study50.
Acknowledgement
Authors are thankful to the Secretary, DHR and Director General, Indian Council of Medical Research for permission and encouragement. Authors are also thankful to various medical and health institutions across the country for providing help at all levels of this project. This study was conducted under Sanofi Pasteur grant no. (---------) for which the authors are grateful.
See the REFERENCES for this paper here
Browse the Table that are used for Article here - PDF File
To be continued..
* Dr. Laishram Ranbir Singh (MD, FIAP, WHO Fellow) is a Professor and Head, Department of Pediatrics, at the Regional Institute of Medical Sciences (RIMS), Imphal Manipur.
He contributes to e-pao.net regularly and can be contacted at drranbirlai(aT)yahoo(doT)co(doT)in
This paper was webcasted at e-pao.net on 11 August 2015.
* Comments posted by users in this discussion thread and other parts of this site are opinions of the individuals posting them (whose user ID is displayed alongside) and not the views of e-pao.net. We strongly recommend that users exercise responsibility, sensitivity and caution over language while writing your opinions which will be seen and read by other users. Please read a complete Guideline on using comments on this website.


