




Epidemiological analysis and patterns of disease amongst patients hospitalized with dengue infection across different hospitals in India
- Part 2 -
Dr. Laishram Ranbir *
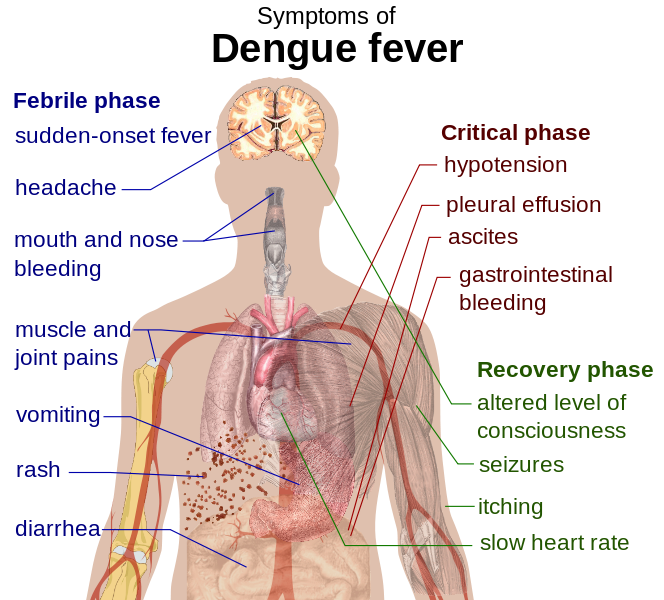
Main symptoms of dengue fever :: Pix - Wikipedia/Mikael Häggström
B.K. Tyagi.1, S. Karthigai Selvi 1, C. Vidya 1, T. Mariappan 1, P. Philip Samuel 1, R. Paramasivan 1, Mukul Gaba 2, N.K. Arora 2, S. Vivek Adhish 3, Deoki Nandan 3, Donald S. Shepard 4, Yara Halasa 4, Harish K. Pemde 5, Anurag Tomar 6, Poovazhagi Varadarajan 7, Pawan Kumar 8, Ashok Mishra 9, V.K. Srivastava 10, Koushik Vyas 11, Ranbir L. Singh 12, Bhadresh R.Vyas 13, Pallavi Shelke 14
1 Centre for Research in Medical Entomology (ICMR), 4-Sarojini Street, Chinna Chokkikulam, Madurai 625002, TN, India (Email: [email protected])
2 National Institute of Health & Family Welfare, Munirka, New Delhi
3 INCLEN Trust International, Okhla Industrial New Delhi
4 Brandeis University, 415 South Street, MS 035, Waltham, MA, USA
5 Lady Harding Medical College, New Delhi
6 NIMS Medical College, Rajasthan
7 Madras Medical College (Institute of Child Health), Tamil Nadu
8 Kasturba Medical College, Karnataka
9 G.R. Medical College, MP
10 IIMS R, UP
11 SCB Medical College, Odisha
12 RIMS, Manipur
13 M.P.Shah Medical College, Gujarat
14 LTM Medical College & General Hospital, Maharashtra
Correspondence to
Dr.B.K.Tyagi
Centre for Research in Medical Entomology (ICMR),
# 4, Sarojini Street, ChinnaChokkikulam,
Madurai-625 002, Tamilnadu, India.
Tel: + 91 452 2520565;
Fax:+ 91 452530660.
Email:[email protected]
Case definition
The World Health Organization (WHO) grading system was used to classify patients infected withdenguevirus32. Dengue fever was divided into classic dengue fever(DF) and dengue fever with haemorrhagic manifestations (DHF) and dengue shock syndrome (DSS).
(1) Suspected DF: Documented fever of >- 38°C or history of fever lasting 27 days with two or more of the following symptoms or signs: headache, rash, retro-orbital pain, myalgia, arthralgia, haemorrhage, hypotension, hemoconcentration (haematocrit elevated ≥ 20% of population mean), thrombocytopenia (platelet count < 100,000 platelets/mm 3 ).
(2) Probable DF: A case of suspected dengue with anti-dengue IgM sero-conversion or single anti-dengueSupportive serology (reciprocal haemagglutination-inhibition antibody titre, comparable IgG EIA titre or positive IgM antibody test in late acute or convalescent-phase serum specimen).
According to WHO guidelines, a confirmed dengue/DHF/DSS must fulfill, apart from clinical description, the laboratory confirmed investigations with one or more of following:
o Isolation of the dengue virus from serum, plasma, leukocytes, or autopsy samples.
o Demonstration of a fourfold or greater change in reciprocal IgG or IgM antibody titres to one or more dengue virus antigens in paired serum samples.
o Demonstration of dengue virus antigen in autopsy tissue by immunohistochemistry or immunofluorescence or in serum samples by EIA.
o Detection of viral genomic sequences in autopsy tissue, serum or CSF samples by PCR.
In India, laboratory criteria of Isolation of dengue virus/demonstration of fourfold change/detection of viral genomic sequence is not being performedto confirm DF/DHF/DSS, hence all the patient with provisional discharge diagnosis of DF/DHF/DSS in Indian scenariowere reclassified as suspect and probable dengue as per WHO's guidelines.
Statistical analysis
Statistical analysis was performed byusing SPSS (version 16). Descriptive statistics were calculated for all relevant variables. Differences between several groups of patients were evaluatedusing Chi-square test or Fisher's exact test for categorical variables and T-test for mean comparison of continuous variables. Relative Risk (RR) was calculated to evaluate the risk exposure between two categorical variables. Multi and univariate regression analysis may be added.
Results
Disease Presentation
Of the total 1450 hospitalized cases admitted during 2006-2011, about 1219 (84.07%), 143(9.86%) and 88 (6.07%) had provisional discharge diagnosis of DF, DHF and DSS respectively were recruited for this retrospective study. Then, reclassification of diagnosis was doneafter examining all the selected medical records carefully on the basis of WHO guidelineswith regard to clinical criteria and fulfillment of laboratory test,where there are about 567 (39.10%) had dengue suspectand remaining 883 (60.90%) had probable dengue(Table 2).
The highest number of hospitalized dengue cases (Suspect & Probable)was reported during the year 2009 and 2010 with303 and 308, mortality rate of 4.62 and 1.95 respectively (Table 3). About 9.60% and 23.37% of the admitted dengue cases had severe bleeding and shock. Among the hospital sites, about 41.17% of dengue cases were reported at southern region. The highest number of hospitalization and death due to denguehas occurred during pre andpost monsoon which goes along with seasonal trend of dengue. A gradual increase was noticed from June with a peak in October for the study year (2006-2011) (Fig. 2).
Socio-demographic characteristics
Tables 4 and 5 summarize the socio-demographic characteristics of the hospitalized dengue cases study site wise and region wise.Sex ratio for dengue cases for male to female was 1.78:1 (64% and 36%, respectively). In region wise also, male was predominantly affected by dengue infection than female. The data collected from two pediatric hospitals (n=581) indicated that number of cases in the age group of 0-1, 1-4 and 5 and above years were 76 (13.08%), 140(24.10%) and 365 cases (62.82%) respectively in which the high incidence of 10.53% of dengue death was reported among the infants (0-1 years).The mean age for dengue suspect and probable was 6.98 and 6.15 years, respectively.
The data collected from the general hospitals revealed that a maximum number of 481(55.35%) cases were hospitalized in the age group 15-44 whereas about 256 (29.45%) casesbelong to the age group of 0-14 years. The mean age for dengue suspect was observed as 25.02 years, and dengue probable as 25.59 years. It indicates that the adults were infected eccentrically to that of children. This pattern was also apparent in the study conducted in Karnataka33. Though geriatric population (age >60) has reported 35 (4.03%) cases of hospitalizationthere was a high mortality rate of 14.29%. Thus the geriatric population is also being at equal risk to that of children in terms of dengue mortality.
The pediatric age group 0-14 was being highly affected by Dengue in North region compared to other regions in India whereas the adult age group (above 14 yrs) was largely affected compared to children across all regions in India. It was found that distribution of dengue disease was also equally prevalent among the rural population compared to urban population in India which varies across regions. The Southern region has reported high number of cases hospitalized from rural areas to that of other regions in India.
Duration of Illness and Utilization of health care services
Table 6 and 7 depicts the duration of illness and patient illness attributes. On average, duration of illness before hospitalization took place in the study sites (tertiary care units) lasted for 6.51 days including an average of 2.71 days of hospital stay and 1.37 days of ambulatory visitswhich may have taken place either at primary or secondary health care facilities. Only 152 (10.48%) cases sought health care facilities within 48 hrs from onset of the disease. The average duration of hospitalization for Dengue suspectand Dengue probable was observed as 4.90 and 6.16 nights respectively. The average total duration of illness until discharge was noticed as 10.89 and 13 days for dengue suspect and dengue probable, respectively. There was significant difference found in duration of illness before admission into study sites (tertiary care units), duration of hospitalization and total duration of illness among dengue suspect and probable.
Clinical Characterization
Table 8 shows the clinical characteristics of the hospitalized dengue cases. It was observed that there was similarity in signs and symptoms amongst dengue suspect and dengue probable except for redness of skin, redness of eyes, myalgia, abdominal pain, diarrhea, nausea, vomiting, hematemesis, malena, bleeding, shock, and pedal edemawhere myalgia and pedal edemawere highly significant and present in Dengue probable.
The common symptoms seen for 1450 cases were fever (99.17%), vomiting (87.05%), generalized body pain (79.33), headache (74.51%), abdominal pain (61.80), liver enlargement (59.30%), myalgia (57.38%), Arthralgia (47.88%), pleural effusion (42.29%), spleen palpable (37.27%), shock (30.49%), facial flushing (26.95%), retro-orbital pain (26.94%), pedal edema (24.32%), Petechiae (22.89%), Malena (20.83%), haematemesis (16.63%) and Severe bleeding (10.62%). History of abdominal pain was the most common complaint contributing to 61.80% where67.38 % and 58.74% was contributed by dengue suspect and dengue probable, respectively. Liver enlargement was also observed in dengue patients (59.30%); 58.70% for Dengue suspect and 59.58% for Dengue probable. Shock was found in 37.41% and 26.22% among suspect and probable dengue and in overall, shock was observed in 30.49% of hospitalized dengue cases.
Dengue probable was more likely to get the signs and symptoms of arthralgia, myalgia, liver enlargement and pedal edema than the dengue suspect. It was observed that the classical signs and symptoms of dengue infection was also highly seen in dengue suspect because about 6% of the dengue suspect cases had died within 1-2 days of admission in the hospitals before undergoing confirmatory laboratory test and about 60.32% of dengue suspect with the clinical discharge diagnosis of DF/DHF/DSS without laboratory diagnosis being done.
Table 9 presents a summary of key clinical features, and basic laboratory findings comparing children (0-14) and adults (>14).The mean age for paediatric patients was 6.18 years. Most adults were between thirties and forties (mean age 31.87 years). Facial flushing, petechiae, altered level of consciousness, abdominal pain, shock, liver and spleen palpable, pleural effusion, ascites, pedal edema were more common amongchildren as disease presentation and also they are being at high risk of getting these signs and symptoms when compared to adult population.
See the REFERENCES for this paper here
Browse the Table that are used for Article here - PDF File
To be continued..
* Dr. Laishram Ranbir Singh (MD, FIAP, WHO Fellow) is a Professor and Head, Department of Pediatrics, at the Regional Institute of Medical Sciences (RIMS), Imphal Manipur.
He contributes to e-pao.net regularly and can be contacted at drranbirlai(aT)yahoo(doT)co(doT)in
This paper was webcasted at e-pao.net on 06 August 2015.
* Comments posted by users in this discussion thread and other parts of this site are opinions of the individuals posting them (whose user ID is displayed alongside) and not the views of e-pao.net. We strongly recommend that users exercise responsibility, sensitivity and caution over language while writing your opinions which will be seen and read by other users. Please read a complete Guideline on using comments on this website.


